by Hamilton E. Davis
It was about this time of year in 2011 when Vermont’s health care reform project was born. The Harvard professor William Hsaio was ready to bring his plan for a radical new delivery system into the Legislature. The plan had been commissioned in the final years of the Douglas administration, but a new governor, Peter Shumlin, had been elected the previous November. Hopes were high for the Hsaio plan because it was a so-called Single Payer proposal, and Shumlin had won both a difficult primary election and a very close general on the strength of his support for exactly such a policy.
However, the Hsaio plan died a quick death, and Shumlin turned the problem over to a new architect, Anya Rader Wallack, and a new political manager, the former lobbyist Steve Kimbell. Working with the Legislature, the Shumlin team came up with a new plan that passed quite easily given its far-reaching significance, and went into effect on July 1 of that year.
At the time, I wrote an analysis for VTDigger suggesting that the Shumlin reform effort could succeed, but that it would have to travel a very long road to get there. In fact, the road has been longer than I expected, and far more difficult than I anticipated. Yet, here we are—close to a financially and medically sustainable reform system. We can now see what such a system looks like but getting there will be very hard. We will begin to see just how hard by the legislative crossover deadline in early March. Over the last couple of weeks, the reform technocrats have been trekking up to the state house to tell legislators where they think we are and where reform is headed. I have very little confidence in that process, partly because after watching it for the last eight years I have seen no evidence that the Legislature understands health care at all; and further, because the press, a.k.a VTDigger, has done a terrible job writing about it, a view I have already expressed at length. In any event, herewith my take on the reform effort:
What has Reform Accomplished So Far?
The reform effort has done two critical things so far. The first is that it has effectively cut annual inflation in the 14-hospital Vermont delivery systems in half. The graph below shows that progress. The graph shows an inflation rate of 8.0 percent over the period 2001 to 2009. I call the rate in 2010, 2011 and 2012 the anomaly period; the drop in 2010 was clearly caused by a drop in demand flowing from the 2008 financial crash, and the 2011 and 2012 rates were set by the Legislature as part of the transition to the establishment of the Green Mountain Care Board.
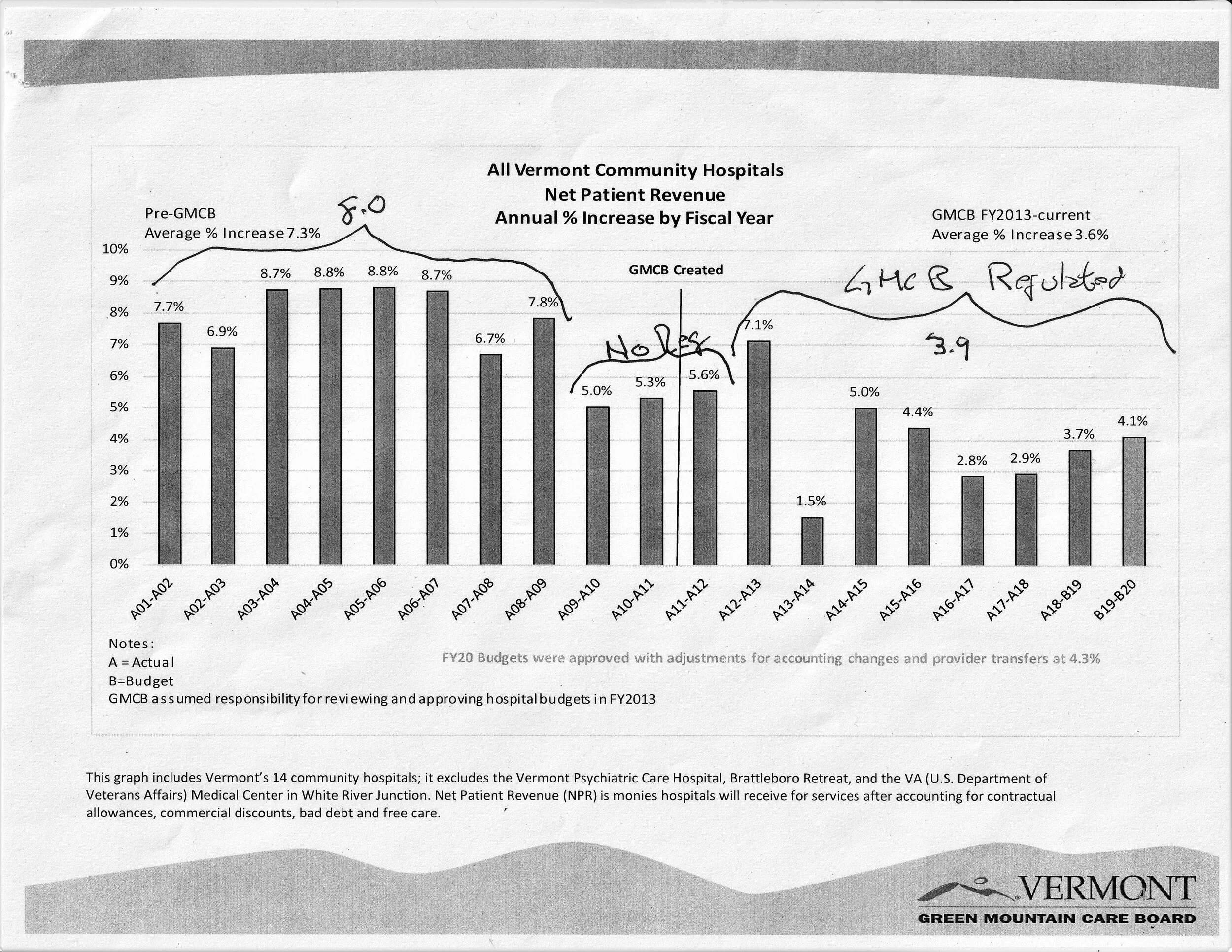
The important number today is an inflation rate of 3.9% from 2013 to the current year. Those gains resulted almost entirely from conventional downward regulatory pressure on hospital spending, although the situation among the small hospitals is unsettled, about which more later. The second major accomplishment of the project is the establishment of OneCare Vermont, the consortium of doctors and hospitals whose purpose is to allow those providers to deliver a full range of care to large cohorts of Vermonters for a fixed price. The key words there are fixed price.
The consensus in the health policy community is that changing how doctors and hospitals get paid is the key to moving health care costs from super-heated inflation that took health spending from 6.6 percent of the U.S. Gross National Product in 1966 to more than three times that today. The fee-for-service engine that has driven spending has to be changed. The knotty question at the heart of health reform is—how?
What’s Going on with OneCare?
No single entity has been more vilified over the course of the reform gauntlet than OneCare Vermont, the state’s single Accountable Care Organization. The only possible exception is the University of Vermont’s health network; and, in fact they should probably be considered together, because much of the opprobrium that flows over OneCare is really aimed at UVM, which is a co-owner. The result is that neither the public nor the legislature have been able to get a fix on it. So, the basic questions:
What exactly is an ACO, and what good is it? An ACO is simply a corporate structure, roughly akin to a cooperative or coalition, that allows a group of doctors and hospitals to provide necessary care to a big bunch of patients for a single price. Consider Sally Smithers, who might live in Swanton. If she has a medical problem, she could go to her primary care doctor, who might solve the problem. If not, the doctor could send her to the community hospital in St. Albans, and if the doctors there couldn’t fix it, they could send her to to UVM Medical Center, or to Dartmouth-Hitchcock, or both, or somewhere else. In fact, patients pinball through the system like that all the time. The ACO simply draws a line around all those hospitals, and establishes a single price for the care they provide. At the same time, it encourages the elements in the system to work together to solve the basic problem—returning Sally Smithers to full health. We need the ACO to accomplish the Vermont reform plan, which gets patients like Sally back to health more efficiently medically, and at a price we can afford.
But why is OneCare, our ACO, doing so badly? It isn’t doing badly; it’s doing just fine. In fact, basically every important piece of data bearing on its performance has been positive. To pick just one: The OneCare budget for 2020 showed that in 2018, just eight percent of the enrolled Medicaid patients were in fixed price contracts, as opposed to the much softer cap of the group cost targets covering the remainder of the Medicaid population. The naysayers and reform opponents jumped all over that—a clear portent of failure they said. But then the 2020 figures came out, and they showed a 10-fold increase, from eight percent to 88 percent. Another positive metric: Vermont Blue Cross, which either insures or manages the health insurance for just north of 200,000 residents, announced recently that they would attribute all of their patients to OneCare. That cohort is not yet enrolled in fixed price contracts, but that’s where they are headed.
Finally, one of the most important metrics ever has just become available. The Medicaid figures for 2018 showed that the fixed price component of spending for that year was set by contract on Jan. 1 of that year at $67,254,681. Facing that discipline, the state’s hospitals and some independent physicians brought that cohort in at $59,591,372, which is $7.7 million below what was expected. The significance of that number demonstrates the potential for fixed price contracting to save real money—the percentage under was 11.5 percent—across the single most important sector of heath system costs. This is a very complex subject, which I will get into more fully in my next post, but it is striking how much is going right with reform now.
I don’t wish to seem Pollyanna-ish about this; there some issues out there, like the total number of Vermonters enrolled across all payers, which is not yet up to scale, but that challenge is manageable. The fact is that OneCare is now fully in place and operational, and while it is not perfect, it is going as well as the other major players, like the Green Mountain Care Board and the Scott administration. Those three pieces of governmental machinery are not obviously parallel things, but they all have to play well and play together to accomplish the reform goal.
As I said at the outset, however, the easy money has already been made. Getting the system fully sustainable will be far more difficult. The last 15 percent of a very heavy lift like health care reform is always the hardest, and so it will be here. And none of the players is really ready for the final push yet. My tiny corps of brilliant readers will note that I haven’t described what the final push will look like, but it is coming—soon.